Article Text

Abstract
Objective To assess the safety and quality of baseline screening colonoscopy in a randomised controlled trial (RCT).
Methods A population-based RCT with an explanatory design is ongoing to evaluate the efficacy of colonoscopy screening in 9751 men and women aged 40–74 years at average risk of colorectal cancer (CRC) in Japan. Screening colonoscopies for the intervention group were performed from June 2009 to June 2017.
Results Of the 4861 participants in the intervention group, 4495 (92.5%) underwent screening colonoscopy. The quality of bowel preparation was excellent (34.8%) or good (45.6%) in 80.4% of cases. The caecal intubation rate was 99.7% (4483/4495), and the mean (±SD) withdrawal time was 9.7 (±5.3) min. The adenoma detection rate (ADR) was 39.4% (1770/4495). A total of 27 participants (0.6%) were diagnosed with CRC, and 266 (5.9%) were diagnosed with advanced neoplasia (AN). In women, adenomas were more frequently detected in the proximal colon than in the distal colon (proximal: 18.9% vs distal: 16.4%, p=0.024), and a similar trend was observed for AN (proximal: 2.4% vs distal: 1.5%, p=0.045). No serious adverse events related to screening colonoscopy were reported, and minor adverse events were observed in two participants (0.04%).
Conclusions Adequate performance in compliance, ADR, and safety was confirmed in the intervention arm of the RCT evaluating the efficacy of screening colonoscopy. The high quality of screening colonoscopy observed in the trial suggests its feasibility as a population-based screening approach.
Trial registration number UMIN000001980.
- COLONOSCOPY
- COLORECTAL CANCER
- COLORECTAL CANCER SCREENING
Data availability statement
Data are available upon reasonable request. All analyses relevant to the study are included in the article. All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The potential efficacy of colonoscopy screening has been reported in observational studies, but definitive evidence from randomised controlled trials (RCTs) is still pending.
Compliance, adenoma detection rate (ADR), and harms of colonoscopy screening in RCTs with explanatory trial designs remain unclear.
WHAT THIS STUDY ADDS
Compliance with colonoscopy screening was 92.5%, and the ADR was 39.4%. Minor adverse events were observed in 0.04% of participants in this RCT with an explanatory trial design.
Advanced neoplasia and adenomas were more frequently located in the proximal colon in women.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The high ADR, low adverse event rate, and high compliance support the feasibility of colonoscopy in population-based CRC screening and its potential to inform future public health policy.
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer-related death, with approximately 2.17 million new diagnoses and 1.09 million deaths reported worldwide annually.1 Screening for CRC is an essential public health strategy to reduce CRC-related mortality. Current CRC screening methods include stool-based tests and imaging evaluations, such as endoscopy. Several randomised controlled trials (RCTs) of guaiac faecal occult blood test (gFOBT) screening showed a 13–33% reduction in CRC mortality rates.2–4 The faecal immunochemical test (FIT) is the first choice for stool testing5 because it has higher sensitivity than gFOBT6 and has demonstrated mortality-reduction effects in several observational studies.7 8
Stool-based screening reduces mortality through early cancer detection, whereas endoscopic screening reduces mortality and incidence by facilitating the removal of premalignant lesions. Several RCTs have shown that sigmoidoscopy reduces the CRC incidence by 18–26% and the mortality by 22–31%.9–13 Colonoscopy is considered more effective than sigmoidoscopy because it can examine the entire colon, and several cohort and case–control studies have reported reductions in CRC incidence and mortality.14–21
Nonetheless, colonoscopy incurs high costs and risks of complications. Therefore, RCTs are necessary to carefully assess the balance of the benefits and harms of colonoscopy screening. Several large population-based RCTs evaluating colonoscopy are ongoing, though final results have not yet been reported.21–25 There is insufficient direct evidence from clinical trials to determine the most desirable screening method when considering the benefits and harms. Japanese and European screening guidelines recommend FIT, but not screening colonoscopy.5 26 27
The Akita Japan population-based colonoscopy screening trial (Akita pop-colon trial) is a population-based RCT conducted in Japan to evaluate the efficacy and safety of a screening method that adds a single colonoscopy to FIT to mitigate CRC incidence and mortality rates. In this report, we describe the adherence rate to screening colonoscopy, baseline characteristics of participants, quality and safety of colonoscopy, and the sex- and age group-stratified proportion of the detected lesions.
Methods
Research design
The Akita pop-colon trial is an ongoing RCT comparing the mortality rate of CRC between an intervention group, which receives a one-time colonoscopy and annual FIT, and a control group, which receives only an annual FIT. Details of the target population and the trial design are described elsewhere.28 The primary endpoint is CRC mortality after a 10-year follow-up. Secondary endpoints include CRC incidence, sensitivity and specificity, and harm (pain and adverse events associated with the screening). As of 2025, the trial is in the follow-up phase, with data collection for the primary endpoint ongoing. Final analyses will be conducted after the planned follow-up period. Participants were men and women aged 40–74 years residing in a defined area of Akita Prefecture, Japan. All interventional colonoscopies were performed at fixed facilities (Kakunodate Hospital or Akita Red Cross Hospital). FIT had been performed as a population-based screening in this area, whereas colonoscopy had not been conducted. The research protocols were approved by the ethics committees of the research organisations, and written informed consent was obtained from all participants after providing a complete explanation of the study. This study adheres to the CONSORT and STROBE reporting guidelines (online supplemental file 2 and online supplemental file 3).
Supplemental material
Supplemental material
Randomisation
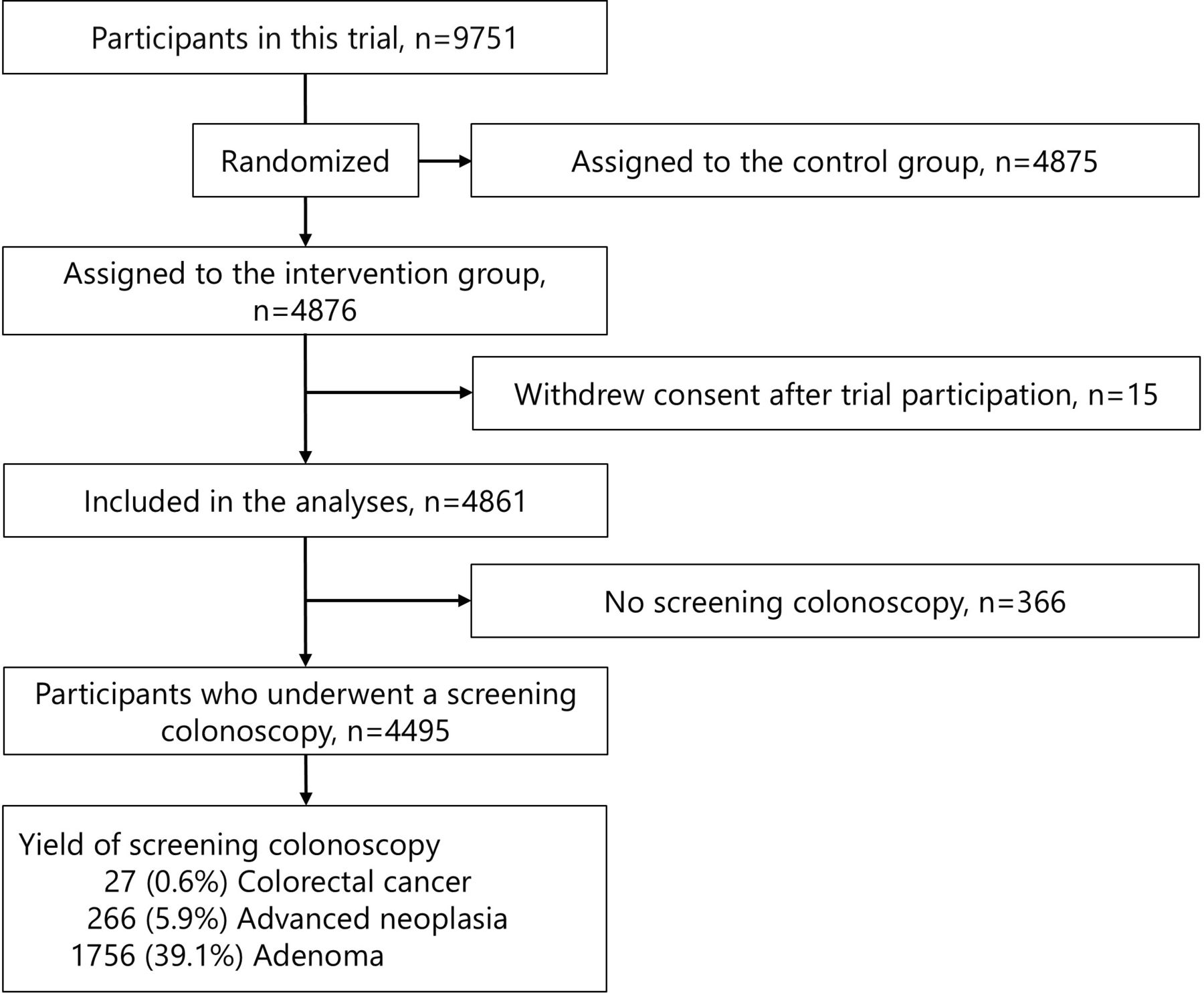
Participant recruitment was conducted at population-based screening sites. Participants who consented to enrol in the trial were randomly assigned 1:1 to either the intervention or control group (figure 1). Participants assigned to the intervention group were briefed about colonoscopy at these screening sites. Within 1 week of trial entry, the designated colonoscopy facilities contacted the participants in the intervention group to invite them to undergo intervention colonoscopy within the next 4 months and scheduled colonoscopy appointments. Participants who could not be screened within 4 months for any reason were permitted to undergo screening colonoscopy as an intervention up to 6 months after study entry. Participants were aware of their group allocation, as blinding was not possible due to the nature of the intervention.

{kind=link}
Flowchart of screening colonoscopy in the intervention group.
Screening colonoscopy
Screening colonoscopy for the intervention group was performed from June 2009 to June 2017, at no cost to the participants. The 52 endoscopists who performed screening colonoscopies for the trial had previously performed at least 200 colonoscopies and were classified into three categories based on their experience: 200–499, 500–4999, and ≥5000 colonoscopies performed. Bowel preparation was performed using a same-day dosing regimen following the protocol. The quality was evaluated on a 4-point scale (excellent, good, fair, and poor) using a modified Aronchick scale.29 All examinations were conducted using a high-definition video colonoscope. At Kakunodate Hospital, standard air insufflation was used until June 2010, and carbon dioxide (CO2) insufflation was used thereafter. At Akita Red Cross Hospital, all colonoscopies were performed under CO2 insufflation. Screening colonoscopies in the intervention group were performed solely for the detection and documentation of lesions; endoscopic treatment or surgery for neoplastic lesions larger than 5 mm was performed at a later date. Colonoscopy information, including detected lesions, was documented in the trial’s dedicated case report form (CRF). CRF information was electronically coded at the local data centre and transmitted to the central data centre for storage.
The lesions were classified into three categories—‘cancer’, ‘adenoma’, and ‘others’—based on endoscopic diagnosis. Other lesions, including serrated lesions (hyperplastic polyp, sessile serrated adenoma/polyp, and traditional serrated adenoma), were noted in the free-text field. Adenomas measuring more than 10 mm or cancers were counted as advanced neoplasia (AN). The diameter, site, morphological classification, and pit pattern of all lesions were documented. The ‘proximal colon’ was defined as the region from the caecum to the splenic flexure, and the ‘distal colon’ was defined as the region from the descending colon to the rectum.
The occurrence of adverse events on the screening day was reported by CRF for all screening colonoscopies. Hospitals were required to report adverse events occurring after the date of colonoscopy to the central data centre on a dedicated form, immediately for serious events, and within 30 days of occurrence for minor events. An adverse event was defined as ‘any untoward or unintended sign, symptom, or disease that occurred after the start of the clinical trial’. A serious adverse event was defined as (1) death, (2) life-threatening event, (3) requiring hospitalisation (initial or prolonged) for treatment (blood transfusion or surgical procedures), (4) resulting in disability or permanent damage, and (5) causing congenital anomaly/birth defect. Mild vagal reflexes that did not need additional treatment were not required to be reported as adverse events. Abdominal pain experienced by the examinee immediately after the screening colonoscopy was assessed using a questionnaire on a 5-point scale: no pain, little, moderate, severe, and extreme. All examinees were instructed to complete the questionnaire and return it to the data centre.
Statistical analysis
The proportions of participants per baseline characteristics were calculated, with the denominator being the total number of participants in the intervention group. The proportions of quality indicators of colonoscopy and detected lesions were calculated according to the sex and age group, with the denominator being the number of screening colonoscopy examinees. The number needed to screen (NNS) for cancer and AN detection was calculated as the inverse of each detection rate. The proportion of cancer, adenoma, and AN detection in the distal or proximal colon was calculated by sex and age group, and a Fisher’s exact test was performed. The adenoma detection rate (ADR) was calculated for each category of endoscopist experience.
For all analyses, a two-sided p value less than 0.05 was considered statistically significant. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Windows, V.28.0 (IBM, Armonk, New York, USA).
Patient and public involvement
None.
Results
Research population
A total of 9751 participants were enrolled in the trial, and 4876 assigned to the intervention group. In the intervention group, 15 participants withdrew consent after enrolment, resulting in a final total of 4861 participants included in the study (figure 1). Baseline characteristics of the participants in the intervention group are shown in table 1.
Baseline characteristics
There were 2526 women (52.0%) and 2335 men (48.0%) with a mean age (± SD) of 58.8 (± 9.3) years. Among the participants, 81.3% had previously undergone CRC screening (88.9% had a FIT, and 7.9% had a colonoscopy). A family history of CRC in first-degree relatives was noted in 10.3% of participants.
Screening participation and colonoscopy indicators
Of the 4861 participants in the intervention group, 4495 (92.5%) adhered to the protocol and underwent a colonoscopy for screening (table 2). The proportions of men and women who underwent colonoscopies were 91.9% and 93.0%, respectively, with the highest proportion in the 50 and 59 age group (94.6%). The overall caecal intubation rate was 99.7% (4483 of 4495), and the mean (SD) withdrawal time was 9.7 (± 5.3) min. Sedative drugs were administered to 14.4% (648) of the participants, with midazolam given to 8.9% and diazepam to 5.7%. Antispasmodic drugs were given to 77.5% (3,484 participants), with butylscopolamine administered to 69.4% and glucagon to 8.1%. Analgesic drugs were given to 1.1% (48 participants), with pentazocine administered to 1.1% and pethidine hydrochloride to 0.04% (online supplemental table 1).
Supplemental material
Procedural characteristics of screening colonoscopy
The quality of bowel preparation was excellent in 34.8% and good in 45.6% of the participants, with more than 80% evaluated as adequate. 52 endoscopists performed the screening colonoscopies. 16 (31%) endoscopists had prestudy experience of 200–499 colonoscopies and performed a total of 586 (13.0%) colonoscopies in the trial. 26 (50%) endoscopists had experience of 500–4999 colonoscopies and performed 3174 (70.6%) procedures, while 10 (19%) endoscopists had experience of ≥5000 colonoscopies and performed 735 (16.4%).
Yields of screening colonoscopy
Table 3 shows the lesions detected in the 4495 participants who underwent screening colonoscopy, categorised by sex and age group. 27 participants (0.6%) were diagnosed with CRC during screening. Of these, 11 participants (0.2%) had lesions in the proximal colon, and 16 participants (0.4%) had lesions in the distal colon. Colorectal polyps were detected in 1988 (44.2%), adenomas in 1756 (39.1%), AN in 266 (5.9%), and serrated lesions in 363 participants (8.1%).
Diagnostic yield at the screening colonoscopy
The total ADR, combining adenoma and CRC, was 39.4% (1770/4495). The ADR by endoscopist experience was as follows: 200–499, 40.1%; 500–4999, 37.1%; and ≥5000, 48.4%. Fisher’s exact test was used to evaluate the difference in the prevalence of adenomas, ANs, and CRC between the proximal and distal colon. In total, there was no statistically significant difference between the proximal and distal colon for any lesions. However, the results of Fisher’s exact test for each sex and age group showed that proximal adenomas were more prevalent in women (proximal: 18.9% vs distal: 16.4%, p=0.024) and in those aged over 70 years (proximal: 35.0% vs distal: 28.4%, p=0.021). Distal adenomas were more prevalent in the 40–49 years group (proximal: 10.8% vs distal: 15.7%, p=0.005). Proximal AN was more prevalent in women (proximal: 2.4% vs distal: 1.5%, p=0.045), while distal CRC was more prevalent in the 50–59 years group (proximal: 0.08% vs distal: 0.65%, p=0.039). No other statistically significant differences were found between sex or age groups. The NNS for CRC was 166.5, and the NNS for AN was 16.9. Regarding morphological classification, polypoid and non-polypoid lesions were found in 25.2% and 28.4% of the participants, respectively. Details of other detected lesions are shown in table 3.
Adverse events
No serious adverse events related to colonoscopy were reported within 30 days of the screening. Minor adverse events occurred in two participants (0.04%). One participant experienced severe abdominal pain after completion of the colonoscopy and underwent an abdominal X-ray and CT scan to assess the risk of perforation. The other participant experienced persistent abdominal pain and visited the emergency room 2 days after the colonoscopy. Both participants showed no other abnormalities and subsequently recovered. Although several transient vagally mediated events, such as bradycardia and hypotension, were observed, all participants recovered quickly after monitoring and did not require additional treatment; therefore, these cases were not reported as adverse events.
Assessment of endoscopic pain
Pain assessment was conducted among participants undergoing screening colonoscopy. Questionnaires were distributed to all 4495 participants, and 4167 (92.7%) responded by mail at a later date. Among the respondents, 88.6% reported no pain (2,938, 70.5%) or little pain (754, 18.1%) immediately after the colonoscopy. Approximately 7.0% of participants reported experiencing more than moderate pain (table 2).
Discussion
This report presents the results of screening colonoscopy performed in the intervention group within an RCT to evaluate the efficacy of screening colonoscopy. The compliance of screening colonoscopy was sufficient, and adverse events were within the predicted range, indicating the feasibility of colonoscopy as a population-based screening tool. The difference in mortality rates, which serves as the primary endpoint, will be assessed at the end of the trial.
Several large-scale RCTs are ongoing internationally to evaluate the impact of screening colonoscopy on CRC incidence and mortality. The Akita pop-colon trial, one of these trials, is characterised by an explanatory trial design,23 30 where informed consent is obtained from all participants prior to randomisation, as is typical in standard clinical trials. Consequently, the compliance rate for screening colonoscopy in the intervention group was as high as 92.5%. Although this explanatory trial design requires more time and effort for informed consent, especially when conducted on a large scale, it allows for the evaluation of screening colonoscopy’s efficacy with high internal validity and a reduced sample size requirement.
Several other screening colonoscopy RCTs use a management trial design with direct randomisation to the target population and invitation to colonoscopy for individuals assigned to the colonoscopy group. Compared with our trial, the compliance rates for screening colonoscopy are relatively low (42.0% in the Nordic countries, 24.6% in Spain, and 35.1% in Sweden), requiring a larger sample size to detect differences in CRC mortality rates.23 25 31 32 The management trial design aids in evaluating the effectiveness of screening colonoscopy due to its external validity and generalisability to average-risk populations. These trials and the Akita pop-colon trial have different objectives and are scientifically complementary. Recently, the intermediate results of a trial in the Nordic countries were reported,32 showing no statistically significant difference in mortality reduction between the colonoscopy and non-screening groups. One potential reason for this lack of significant difference is the low compliance rate of 42% for screening colonoscopy. However, a difference in incidence was observed at this stage, and further long-term follow-up results are anticipated.
The ADR of screening colonoscopy has been reported to be inversely associated with interval cancer incidence.33 34 The ADR in the Akita pop-colon trial (39.4% overall, 37.1–48.4% per endoscopists’ experience) and caecal intubation rate (99.7%) were adequate. This trial reported the highest ADR (30.7% in Nordic countries, 31.7% in Spain) and caecal intubation rate (96.8% in Nordic countries, 94.9% in Spain, 95.8% in Sweden) compared with other screening colonoscopy RCTs, despite not setting an a priori quality control threshold.22 31 32 35 There is evidence that ADR is improved with a 9-minute withdrawal time compared with 6 min.36 The sufficiently long withdrawal time in our trial (mean 9.7 min, median 8 min) may have contributed to the improved ADR. These results are encouraging for accurately assessing the efficacy of screening colonoscopy. Detection and removal of adenomas through screening reduce CRC incidence, subsequently leading to a reduction in CRC mortality.37 However, a high ADR also increases the frequency of surveillance colonoscopy. Future analyses of this and other trials will reveal whether the impact of CRC on incidence and mortality rates exceeds the increased burden of surveillance colonoscopies.31
Recent discussions have focused on sex differences in the prevalence of lesions in the proximal and distal colon, as well as the efficacy of sigmoidoscopy and colonoscopy. It has been reported that proximal colon lesions are more prevalent in women,38 and the efficacy of screening sigmoidoscopy, which only allows observation of the distal colon, is inferior in women compared with men.39 40 A prospective cohort study on colonoscopy, which enables observation up to the proximal colon, reported similar mortality reduction effects in women and men.20 In our trial, the proportion of AN and adenoma detection in women was significantly higher in the proximal colon than in the distal, consistent with the findings of many previous studies. In contrast, a Nordic trial demonstrated a higher prevalence of lesions in the distal colon in both men and women.31 The high detection rate of lesions in the proximal colon among women in our trial, with its well-controlled explanatory trial design and high caecal intubation rate, may provide a valid answer to these controversies in the future.
No major adverse event was observed in all 4495 screening colonoscopies, and the frequency of minor adverse events was 0.04%. This proportion is lower than that reported in other population-based trials (0.13% in Nordic countries, 0.51% in Spain, and 0.2% in Sweden)22 25 31 32 and is considered acceptable. In many other trials, bleeding associated with polypectomy, which is performed in conjunction with endoscopy, must also be included in the number of adverse events. By restricting screening colonoscopy to observation only in our trial, we were able to assess the pure harm caused by screening alone, excluding the effects of treatment. Furthermore, the lower proportion of sedation use (14.4%) in our trial compared with that in Spain (96%) and Nordic countries (22.7%) may have contributed to the lower incidence of adverse events.
Endoscopic pain may be a barrier to undergoing a screening colonoscopy. In our trial, 88.6% of participants reported no or little pain, and 7.0% reported moderate or greater pain. These figures are comparable to, or slightly lower than, those reported in the Nordic trial and several sigmoidoscopy trials.41 42 Sedation is effective in reducing pain during the examination, and CO2 insufflation helps reduce persistent pain.43 44 In our trial, CO2 insufflation was used in 82.5% of participants, and sedation was used in 14.4%. Screenings by expert endoscopists were limited to 16.4%, thereby maintaining the generalisability of this trial. Our findings indicate that acceptable screening colonoscopy is achievable with CO2 insufflation, even without the active use of sedation.
This report has some limitations. First, the lesions were reported based on endoscopic diagnosis rather than pathology. According to the protocol, the screening colonoscopy in this trial was performed solely to detect and document lesions, with treatment occurring at a later date. At the time this study protocol was developed, endoscopic resection of diminutive adenomatous polyps (<5 mm) was not strongly recommended in Japan, and follow-up was considered an acceptable approach due to concerns about postpolypectomy bleeding and other adverse events. Therefore, this study adopted a policy of treating only polyps ≥5 mm. Since lesions <5 mm were not resected, their pathological confirmation was not possible, and restricting the analysis to treated lesions would have led to an underestimation of the actual lesion prevalence. In addition, with the recent development of AI image analysis technology,45–47 endoscopic diagnoses alone are becoming increasingly important, particularly in cases where immediate histological evaluation is not performed. Therefore, reporting the prevalence of all lesions, including those smaller than 5 mm, based solely on endoscopic findings is valuable. Several reports have documented strong agreements between endoscopic and pathological diagnoses.48 49 In this trial, a magnifying endoscope was used in 97.4% of cases, and we plan to evaluate the agreement between the pathological and endoscopic diagnoses of treated lesions in the future.
Second, the quality of bowel preparation in this trial may have been slightly lower than in other studies. Good or excellent preparation was achieved in approximately 80% in our trial, compared with approximately 90% in the Nordic study and 98.0% in Sweden.25 31 This difference may be attributed to the fact that we did not use a split-dosing regimen for bowel preparation but were limited to a same-day dosing regimen according to the research protocol.50 Poor bowel preparation quality may lead to false-negative results in lesion detection. However, this trial setting is appropriate for evaluating the feasibility of future population-based screening, as split-dose preparation is not always practical when colonoscopy is conducted widely as a population-based screening method. Despite this setting, the higher ADR in this trial compared with other studies suggests that the negative effects of the same-day dosing regimen on lesion detection are not critical.
Third, there is the possibility of participant sampling bias. Participants who were not resistant to screening or colonoscopy may have been more likely to be sampled. This bias is unavoidable in a trial with an explanatory design, as obtaining sufficient explanation and consent for an RCT involving a highly invasive procedure like colonoscopy is an essential ethical requirement. When reporting final results in the future, we may clarify the characteristics of the trial participant population by comparing the incidence and mortality rates with those of non-participant residents in the area.
In conclusion, the Akita pop-colon trial intervention group demonstrated adequate performance in terms of compliance, ADR, and safety during screening colonoscopy. This trial, conducted as an RCT with an explanatory trial design, aims to evaluate the efficacy of screening colonoscopy. The quality of screening colonoscopy reported in this study suggests that colonoscopy is a feasible method for population-based CRC screening and indicates the likelihood of achieving valid final trial results after the planned follow-up.
Data availability statement
Data are available upon reasonable request. All analyses relevant to the study are included in the article. All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Ethics statements
Patient consent for publication
Ethics approval
This study was conducted with ethical approval from the institutional review board of Showa University (Approval No. 0812-02). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors sincerely thank the staff of Kakunodate Hospital and Akita Red Cross Hospital.
References
Footnotes
Contributors Conception and design: S-eK, SY, NH, and HS. Data collection: S-eK, KK, FI, H-oY, KW, and H-oM. Analysis and interpretation of the data: NT, KK, FI, SY, TM, and HS. Drafting the article: NT, KK, and TM. Critical revision of the article for important intellectual content: S-eK, NT, KK, FI, SY, KN, TM, and HS. Final approval of the article: S-eK, NT, KK, FI, H-oY, SY, KN, KW, H-oM, NH, TM, and HS. TM is responsible for the overall content as the guarantor.
Funding This trial was funded by a grant (no. JP23ck0106812) from the Japan Agency for Medical Research and Development (AMED).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.