Article Text

Abstract
Introduction Targeted immunomodulators (eg, advanced therapies) effectively achieve symptomatic remission in patients with inflammatory bowel disease (IBD). However, ~25%–50% of patients with IBD achieving symptomatic remission with an advanced therapy may have continued endoscopically/radiologically active bowel inflammation, and it is uncertain whether changing alternative advanced therapies in asymptomatic patients with IBD will reduce bowel inflammation and achieve durable deep remission.
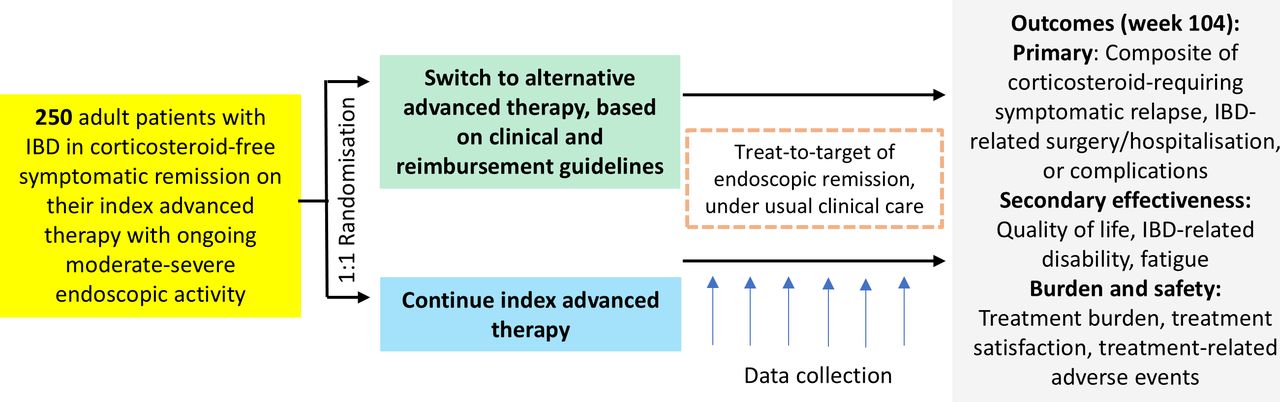
Methods and analysis The QUality Outcomes Treating IBD to Target (QUOTIENT) study is an open-label, multicentre, pragmatic, randomised, controlled trial that aims to compare the efficacy and safety of switching to an alternative advanced therapy targeting endoscopic/radiological remission (treat-to-target) versus continuing the initial, or index, advanced therapy, in asymptomatic patients with IBD with moderate-to-severe endoscopic/radiological bowel inflammation. Enrolment is planned for ~250 participants in Canada/USA, randomised 1:1 to switching to alternative advanced therapy or continuing index advanced therapy, and then followed 104 weeks within routine clinical practice. Patient-reported outcomes measure efficacy and quality of life/treatment burden/safety. Primary endpoint is the time from randomisation to treatment failure.
Ethics and dissemination The study is conducted in compliance with the protocol, ICH Good Clinical Practice, applicable regulatory requirements and appropriate review boards/independent ethics committees (approval numbers: Pro00077486; Pro00061437; STUDY00002062; 22-004171; i22-01269; IRB22-0890; IRB_00154397; 2000032384; SHIRB#2022.095-2; STUDY00007146; MMC#2024-18; REB#125290; 17784; Pro00142214; 20240660-01H), with documented written informed consent. Findings will be disseminated through peer-reviewed journals, scientific presentations, and publicly available Patient-Centered Outcomes Research Institute (PCORI) websites, including lay summaries. The Crohn’s & Colitis Foundation Education, Support, and Advocacy Department, and our patient advocacy stakeholder, will develop educational and marketing resources to communicate findings to a broad audience (>250 000 patients/caregivers/healthcare professionals).
Trial registration number NCT05230173.
- INFLAMMATORY BOWEL DISEASE
- CROHN'S DISEASE
- IMMUNOTHERAPY
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Treat-to-target endoscopic and/or radiological remission is a potential therapeutic strategy that may improve patient outcomes in patients with inflammatory bowel disease (IBD). However, whether treatment should be switched in asymptomatic patients with active inflammation in pursuit of a treatment target of endoscopic and/or radiological remission presents clinical equipoise.
WHAT THIS STUDY ADDS
The QUality Outcomes Treating IBD to Target (QUOTIENT) study is an open-label, multicentre, pragmatic, randomised, controlled trial designed to address this knowledge gap by comparing two treatment strategies of treat-to-target in patients with IBD in symptomatic remission but with significant ongoing bowel inflammation detectable by endoscopy and/or radiology, to determine if a targeted immunomodulator (advanced therapy) switch will reduce bowel inflammation and achieve remission. With a primary endpoint of time from randomisation to treatment failure during 104 weeks of follow-up within routine clinical practice, the trial focuses on comparing two advanced therapy treatment strategies rather than different medications, since the primary question for treat-to-target is treatment modification, not specifically treatment sequencing. We will capture quality of life, treatment burden, and patient satisfaction to discern how patients view two competing advanced therapy treatment strategies.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This pragmatic clinical trial represents a real-world approach for treating patients with IBD and comparing two distinct, yet valid, advanced therapy treatment approaches. This trial focuses on patient-centred outcomes and will directly impact clinical guidelines and practice.
Introduction
Crohn’s disease (CD) and ulcerative colitis (UC), collectively referred to as inflammatory bowel disease (IBD), affect approximately 2.4 million and >320 000 individuals in the USA1 and Canada,2 respectively, cost >$25 billion annually, and cause substantial patient morbidity, diminished quality of life and decreased work productivity.3–5 As a chronic relapsing-remitting disease, treatment goals for patients with IBD involve resolving symptoms, minimising relapses and unplanned healthcare utilisation, and reducing disease-related complications.
Standard treatment of IBD often involves long-term use of potent targeted immunomodulator therapies, referred to herein as advanced therapies, including biologic agents such as tumour necrosis factor-α antagonists, anti-integrins, interleukin (IL)-12/IL-23 and IL-23 antagonists, and small molecule drugs (eg, Janus kinase inhibitors and sphingosine-1 phosphate receptor modulators). These agents have revolutionised the management of IBD; approximately 40%–60% of patients achieve symptomatic remission with these agents and avoid disease-related complications. However, these medications can be associated with side effects increasing the risk of serious infections and certain cancers, including non-melanoma skin cancers and lymphoma.6–8 Advanced therapies are also very expensive and contribute substantially to the rising cost of managing IBD.
While advanced therapies are effective in achieving symptomatic remission, approximately 25%–50% of patients with IBD achieving symptomatic remission with an index advanced therapy (defined as the initial advanced therapy the participants are receiving at the start of the study) have persistent endoscopic evidence of inflammation.9–12 Cohort studies and post-hoc analyses of clinical trials have demonstrated that persistent endoscopic inflammation can substantially increase the risk of clinical relapse, disease-related complications, unplanned healthcare utilisation, and lead to inferior quality of life compared with patients achieving endoscopic remission by resolving bowel inflammation,13–17 which may contribute to patients’ worries and fears about the disease.18 19
Cohort studies suggest 20%–38% of patients with IBD treated with advanced therapies require dose optimisation, with approximately 30%–54% of these patients achieving clinical and/or endoscopic remission.20–22 Consequently, clinical guidelines and expert consensus statements recommend optimisation of index therapy, if feasible, in patients not achieving symptomatic and endoscopic remission targets.23–25 However, despite iterative optimisation of advanced therapy (online supplemental figure 1), approximately 35% of patients with CD and 15% of patients with UC who are in symptomatic remission could be estimated to continue to have significant bowel inflammation.26–29 The Effect of Tight Management on Crohn’s Disease (CALM) trial demonstrated that a treat-to-target strategy, involving treatment escalation when symptomatic and/or objective biochemical targets were not achieved, resulted in improved clinical outcomes compared with symptom-based escalations in therapy only.30 However, it was designed around optimising the index treatment rather than switching to an alternative therapy and did not use endoscopy/radiology as a treatment target. Therefore, patients and providers are often faced with a dilemma as to whether switching to an alternative advanced therapy in asymptomatic patients with ongoing bowel inflammation would be beneficial. With limited evidence on the comparative efficacy of advanced therapies and a lack of predictive biomarkers to personalise the choice of advanced therapies, this empiric treatment switch may inadvertently be a less effective therapy, increasing the risk of relapse and complications, and may still not achieve endoscopic remission. This equipoise represents a key evidence gap in the management of patients with IBD.
Supplemental material
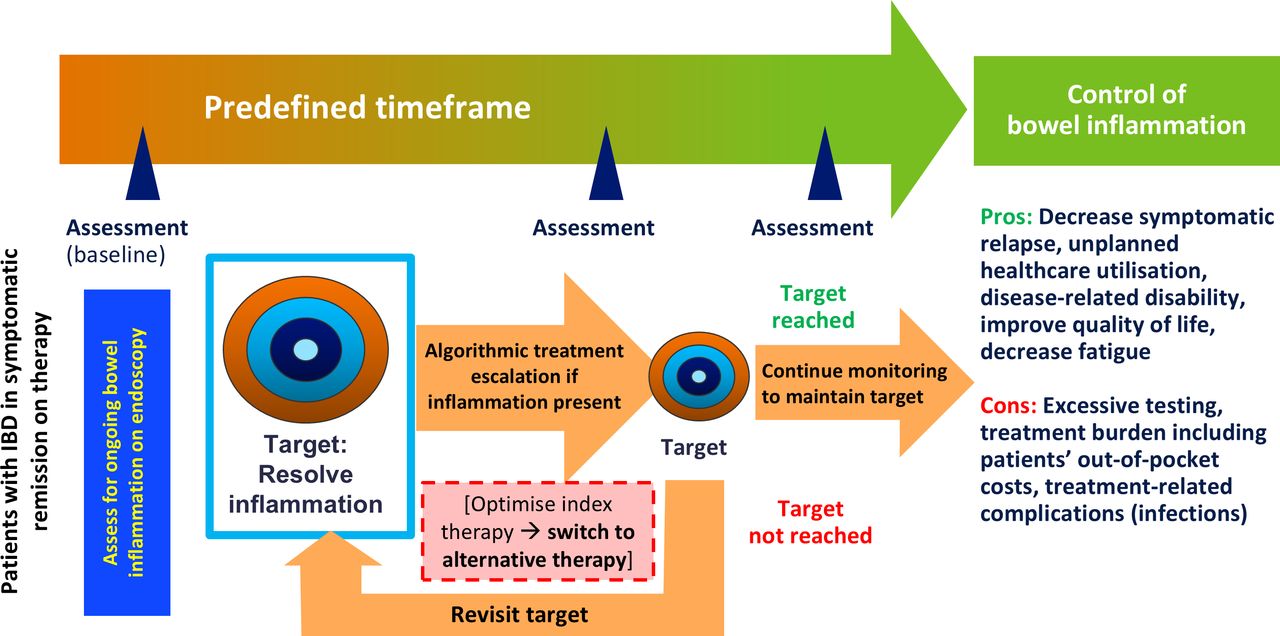
While treat-to-target strategies (figure 1)31 are recommended over a non-targeted treatment approach in other chronic diseases such as rheumatoid arthritis, optimal treatment targets are set at clinical and biochemical remission rather than aiming for complete radiological resolution of inflammation.32 There is considerable variability in IBD guidelines and recommendations, and consequently, practice patterns for treat-to-target in IBD. Some clinical guidelines and expert consensus statements recommend symptomatic and endoscopic remission as preferred treatment targets in patients with IBD, and suggest changing treatment iteratively in order to achieve a target of endoscopic remission.23 25 33 In contrast, other guidelines identify risk-benefit synthesis of targeting symptomatic remission versus incrementally treating to endoscopic remission as a key knowledge gap.24 34–36 Furthermore, there is considerable variability in practice patterns for treat-to-target strategies in the real world.37 Since five classes of advanced therapies are currently approved for managing IBD, switching to an alternative advanced therapy within a treat-to-target paradigm may achieve endoscopic remission in patients with persistent bowel inflammation.38 39 However, the benefits and advisability of switching treatments in asymptomatic patients in real-world practice are unknown. There is a risk that an asymptomatic participant may deteriorate on new therapy when switching advanced therapies, as well as the potential risk of running out of other advanced therapies to switch to if a participant continues to not achieve endoscopic/radiological remission with different advanced therapies.

Core concept of treat-to-target of endoscopic remission in patients with IBD. IBD, inflammatory bowel disease. Source: adapted from Bouguen et al.31
There is a critical unmet need for a real-world, patient-centred evaluation of the efficacy and safety of treat-to-target strategies in patients with IBD. This study protocol describes an open-label, multicentre, pragmatic, patient-centred, randomised controlled trial comparing a strategy of switching advanced therapies to treat to a target of endoscopic/radiological remission versus continuing the index advanced therapy, in asymptomatic patients with IBD with persistent moderate-to-severe bowel inflammation, to assess which approach improves outcomes without increasing treatment burden or adverse events (AEs).
Methods and analysis
Study objectives
The objectives of this study are to compare (1) the efficacy and (2) quality of life and the burden and safety of switching to an alternative advanced therapy to treat to a target of endoscopic/radiological remission versus continuing the index advanced therapy in asymptomatic patients with IBD with ongoing significant bowel inflammation, detectable on endoscopy/radiology. Advanced therapies approved for IBD treatment include biologic agents (eg, tumour necrosis factor-α antagonists; ustekinumab; vedolizumab) and small molecule inhibitors (eg, Janus kinase inhibitors such as tofacitinib; ozanimod), and future advanced therapies that become commercially available during the conduct of the trial.
Study design and population
The QUality Outcomes Treating IBD to Target (QUOTIENT) study is an open-label, multicentre study conducted in asymptomatic patients with IBD who have persistent moderate-to-severe endoscopic or radiological inflammation, and has been designed as a pragmatic trial, using the PRECIS-2 framework (online supplemental figure 2).40 This study plans to enrol approximately 250 participants in the USA and Canada. Patients who meet the inclusion criteria without exhibiting exclusion criteria are eligible to be enrolled in the study (table 1; online supplemental table 1). Participants’ written informed consent is obtained and documented (online supplemental table 2).
Inclusion and exclusion criteria
After randomisation, participants in both treatment arms are followed prospectively within routine clinical care for up to 104 weeks with their treating physician and are scheduled for routine clinical follow-up, either in-person or using telemedicine (eg, phone call/video conference), as per local site practice, at the discretion of their treating physician. A period of 104 weeks was chosen to provide sufficient time for asymptomatic participants to potentially experience an IBD flare or symptomatic relapse. There is no study-mandated visit schedule; however, participant visit schedules will follow local standard of care (SOC) with additional visits at the treating physician’s discretion, and participants are required to complete the patient-reported outcome (PRO) questionnaires at predefined timepoints (table 2). An overview of the study design and schedule of events is provided in figure 2 and table 2. The baseline qualifying endoscopy (or imaging study) can occur within 6 months prior to enrolment, and if multiple endoscopy/imaging procedures were performed in the preceding months, then the most recent qualifying procedure will be captured. The dose of advanced therapy must be stable for at least 3 months prior to the qualifying endoscopy/radiology, and will remain stable between the qualifying procedure and randomisation. No treatment escalation of advanced therapy or addition of immunomodulators, corticosteroids or mesalamines after the qualifying endoscopy/radiology procedure up to randomisation is permitted. The Standard Protocol Items: Recommendations for Interventional Trials checklist is provided in online supplemental table 3.
Schedule of events*

{kind=link}
{kind=link}
Overview of QUality Outcomes Treating IBD to Target (QUOTIENT) study: open-label, multicentre, pragmatic, randomised, controlled trial of treat-to-target strategies in IBD. IBD, inflammatory bowel disease.
This study is patient-centred, with patient-prioritised outcomes. A patient advisory board (the IBD Qorus Patient Advisory Council), which meets quarterly, helped design this study and prioritised clinical status (eg, risk of symptomatic relapse and need for corticosteroids; IBD- or treatment-related hospitalisation, surgery and complications), quality of life (eg, overall quality of life; physical, social, and emotional well-being; fatigue; IBD-related disability), the burden of treatment (eg, financial burden; burden of monitoring; treatment side effects), and treatment satisfaction as outcomes of interest. During the planning of this study, the Patient Advisory Board expressed decisional conflict related to switching advanced therapies, which highlighted their fears about weighing trade-offs of switching therapy with hope of avoiding future complications. Potential risks associated with switching to a new advanced therapy may include worsening of underlying disease activity, potential progression to disease-related complications and/or side effects related to the new advanced therapy. In addition, treatment interruption of an index advanced therapy, while trying an alternative advanced therapy in the treat-to-target paradigm, may render the index therapy ineffective if retreatment is warranted due to the potential development of antidrug antibodies. In contrast, continuing treatment with index advanced therapy in participants with ongoing inflammation may result in ongoing or worsening bowel inflammation that leads to a higher risk of relapse, unplanned healthcare utilisation due to disease-related complications, and inferior quality of life that can lead to other complications. However, all treatment scenarios proposed in this protocol are part of routine clinical care and therefore, the risks and benefits are not different from what would be observed in routine clinical care. Patient-prioritised treatment goals were to (1) achieve remission off corticosteroids while maintaining good quality of life, (2) avoid unpredictable relapses and disability, (3) decrease the risk of hospitalisation and surgery, while (4) minimising treatment burden and (5) avoiding treatment complications.
Recruitment
A total of 29 sites are planned, with currently 6 in Canada (members of the Canadian IBD Research Consortium) and 23 USA sites within IBD Qorus, which is a learning health system built on a collaboration between patients and providers that aims to improve healthcare value for patients with IBD.41 The participating sites are a mixture of academic, single-specialty gastroenterology, and multi-specialty gastroenterology practice centres. Study enrolment began on 5 October 2022; as of 19 December 2024, 88 participants are enrolled and 22 sites are currently recruiting. The expected study completion date is 1 June 2028. During the prescreening process, providers evaluate clinical data related to treat-to-target, including endoscopic remission status, current IBD medications, and plan for treat-to-target of endoscopic/radiological remission. Monthly reports are collected from all sites, and include lists of eligible patients, the number consented/randomised, and of those not consented, why they were excluded including patients’ and/or providers’ preference for making a decision to switch or not to switch.
Randomisation and blinding
Eligible participants are randomly assigned in a 1:1 allocation ratio to one of two treatment strategies, that is, either continuing index advanced therapy or switching to an alternative advanced therapy. Randomisation occurs through a computer-generated, centralised randomisation service with permuted block randomisation of alternating sizes to ensure allocation concealment. Randomisation is stratified by disease phenotype (eg, CD vs UC).
Since this is an open-label study, participants and site investigators are not blinded to treatment allocation. To minimise bias related to open-label design, outcome is adjudicated by blinded outcome assessors.
Study outcomes
The specific objectives and endpoints of the QUOTIENT study are described in table 3.
Planned outcomes and measures
Treatment
Participants in both treatment arms continue routine clinical care with their treating provider, including testing and continuation or discontinuation of any concomitant therapies. Participants randomised to a strategy of switching advanced therapy discontinue their existing advanced therapy and are switched to an alternative advanced therapy approved for management of IBD and covered by the participants’ insurance formulary as part of routine care. Participants may be switched to another medication in the same drug class. Addition of another advanced therapy (ie, dual biologic or biologic combined with advanced oral molecule drug) to an existing advanced therapy does not constitute a switch, since adding another advanced therapy while maintaining treatment with the current advanced therapy is less likely to put the participants at risk of flare. However, for participants on advanced combination therapy, switching one of the advanced therapies with a new advanced therapy, while keeping the other advanced therapy unchanged, is considered a switch. No study-related medications are provided. The selection of an alternative agent is determined at the discretion of the local site physician in accordance with clinical guidelines on management of moderate-to-severe UC and CD23–25 and any updates during the course of the trial. These guidelines include recommendations on the positioning of advanced therapies for first-line use in patients who are advanced therapy-naïve and second-line use in patients with prior advanced therapy exposure.
Participants (and their providers) in either treatment arm are allowed to stop or start new advanced therapies and other IBD-directed therapies in case of symptomatic relapse or intolerance to therapies, at the discretion of the treating provider-patient team.
Medication records of randomised participants are used to assess adherence to the selected treatment strategy, and a medical log is used to document any advanced therapy switches or if the criteria were not met. Fidelity measures are analysed by measuring adherence and non-adherence to the study protocol using a physician-reported survey to assess whether participants were switched to an alternative advanced therapy when randomised to continue the index advanced therapy, and vice versa. Given potential heterogeneity in the advanced therapy switching arm, survey questions include the type of medication switch and reasons for choosing specific medications: (1) participant preference, (2) provider preference, (3) access/cost, and (4) other (with a brief explanation).
Participants are permitted to continue taking, starting or stopping mesalamine, thiopurines, or methotrexate, or adding other advanced therapies to the existing index advanced therapy after randomisation, at the discretion of the treating provider-patient team. If IBD-related medications are added/modified in response to a symptomatic flare (eg, adding corticosteroids/budesonide, immunomodulators, another advanced therapy or dose-escalating existing advanced therapy), the participant will have met the primary outcome. At enrolment, participants cannot be on prednisone (or equivalent); initiation of corticosteroids as rescue therapy for a documented symptomatic IBD flare during the study is considered treatment failure (ie, deemed to have met the primary outcome, as defined in table 3). All participating sites have a standard practice of confirming active inflammation prior to initiation of prolonged courses of corticosteroids, and all oral and/or rectal IBD-related medications (eg, mesalamine, corticosteroids, thiopurines, methotrexate, advanced therapies, etc) received by the participant following randomisation are recorded.
Assessments
Baseline data are collected for the most recent SOC assessments that occurred within 6 months prior to informed consent. Demographic, medical, disease, and surgical history variables are collected at baseline, including age, sex, race and ethnicity, body mass index, smoking status, IBD diagnosis with date of onset, disease location, Montreal classification, major comorbidities, medication history, laboratory and imaging assessments, and prior IBD surgeries.
Participants complete PRO measures electronically, which are used to determine primary (efficacy) and secondary (quality of life, treatment burden and satisfaction) outcomes to determine how participants perceive their condition and its impact on their life. Participants complete the validated 2-item PRO (PRO2) questionnaires at baseline and approximately every 12 weeks during the 104-week follow-up period, which commences after randomisation. The PRO2 UC consists of stool frequency and rectal bleeding subscores of the Mayo Clinic Score, and the PRO2 CD consists of daily stool frequency and abdominal pain score. Additional questionnaires (eg, IBD-Control, Patient-Reported Outcomes Measurement Information System (Fatigue-Short Form 7a), Short Inflammatory Bowel Disease Questionnaire, IBD Disability Index for Self-Report, Treatment Burden Questionnaire, Treatment Satisfaction Questionnaire for Medication, and the Costs for Patients Questionnaire) are completed at baseline following randomisation, and three additional times (at 6, 12 and 24 months) during the 104-week follow-up period (table 2).
Endoscopic disease activity
Endoscopy results are collected if/when performed in the context of routine clinical care; no study-mandated endoscopies will be performed. The baseline qualifying endoscopy must be within 6 months prior to screening without interval treatment change. All endoscopy results are assessed by local readers, including confirmation of eligibility; all site investigators are trained to standardise endoscopy reading.
Participants randomised to switching advanced therapy to pursue a target of endoscopic/radiological remission typically undergo SOC endoscopy to assess resolution of inflammation approximately 6–9 months after the treatment switch, followed by optimisation of switched advanced therapy in case of failure to achieve endoscopic remission. Participants randomised to continuation of index advanced therapy undergo testing for resolution of inflammation at the discretion of the treating provider-participant team.
Completion of endoscopic disease activity assessments are at the discretion of the treating physician and are completed as per local SOC. The endoscopic/radiological remission target is typically assessed in both treatment arms at approximately 26 weeks following study enrolment, with endoscopic remission defined for CD using the Simple Endoscopic Score for Crohn’s Disease score <3 or Simplified Endoscopic Mucosal Assessment for Crohn’s Disease score <2, or resolution of ulcers; and for UC using Mayo Endoscopic Score=0/1. Endoscopic response for CD is also measured, defined as >50% reduction from baseline.
Data collection and management
Data on effectiveness, treatment burden, and safety outcomes, including advanced therapy treatment details, use of IBD-related concomitant medications, laboratory and imaging disease-monitoring assessments, PRO assessments, safety assessments, and health-resource utilisation assessments, are collected from sites by trained site personnel and entered into the electronic data capture system (REDCap)42 database hosted at the Crohn’s & Colitis Foundation. Routine clinical data are collected by the sites at baseline and then approximately every 6 months thereafter, up to a 104-week follow-up period.
In addition, self-reported data from the participants on primary effectiveness outcomes are captured in-between visits every 12 weeks in the patient-facing REDCap survey, through a short five-question survey eliciting clinical, functional status and healthcare utilisation (online supplemental table 4); additionally, at predetermined intervals, more detailed PRO questionnaires are also administered electronically through an email with a link. Paper versions of the questionnaires are available for participants who are unable to use the online versions.
A Data and Safety Monitoring Board has been established for the study and reviews the interim unblinded data every 6 months to monitor safety and effectiveness, and provides recommendations to ensure that participants are not exposed to undue risks. The investigators permit study-related monitoring and audits of the data collection process.
Statistical analyses
Sample size determination
The sample size estimation is based on a primary analysis of time to the first occurrence of a composite event, using methods described by Lachin.43 Based on information from American Gastroenterological Association guidelines, the estimated 1- to 2-year risk of relapse and complications in asymptomatic patients with IBD with significant bowel inflammation is approximately 50%–60%.44 45
The Patient Advisory Board deemed that to overcome their decisional conflict to justify switching advanced therapies, the expected benefit with treatment switching should be a 25%–50% lower risk of relapse and unplanned healthcare utilisation. Hence, with a 104-week control event rate and 5% dropout rate every 6 months, to detect a 36% (eg, the mid-point of the 25%–50% interval) lower risk of experiencing composite outcome measure with intervention for 80% power and two-sided significance level of 5%, assuming a recruitment period of 54 weeks and a total study time of 104 weeks, a total sample size of ~250 participants (randomised 1:1 to intervention and control) would be required. This sample size will provide >80% power to detect a moderate effect size (mean difference divided by SD) of 0.30 in continuous effectiveness outcome measures, which is above the minimal clinically important difference for these outcomes.
Medication switch is assessed to evaluate if the switch is concordant with clinical guidelines, and sensitivity analyses are conducted per protocol, such that no adjustments are made to, after initial randomisation, exclude participants who were switched to an alternative advanced therapy from the continuation arm at their providers’ discretion in the absence of patient-related symptoms, as well as exclude patients in whom a second advanced therapy is added after initial randomisation in either arm. Descriptive analyses of reasons for medication switching that are not concordant with clinical guidelines are performed.
Analyses
The primary analysis is based on all participants who are randomised to a strategy of switching to an alternative advanced therapy to treat to a target of endoscopic remission versus continuing index therapy (full analysis set), in an intention-to-treat (ITT) principle. Participants randomised to switching advanced therapies who are unable to switch due to insurance denial will be analysed in the treatment group they were assigned to, in ITT analysis.
Secondary analyses will be conducted based on the modified ITT (mITT) analysis set (participants randomised to switching who receive ≥1 dose of the alternative advanced therapy). In both the primary and secondary datasets, participants who drop out after randomisation (in ‘full analysis/ITT set’) and receipt of the first dose of alternative advanced therapy (in ‘mITT analysis set’) will be considered censored. Participants randomised to switching advanced therapies who are unable to switch will also be considered censored, in mITT analysis.
Participants will also be analysed in a per-protocol analysis (participants who continue in the group they were allocated to after randomisation, throughout the study until the study end or until they meet the primary outcome, whichever comes first). The per-protocol analysis will exclude participants who were switched to an alternative advanced therapy from the continuation arm at their providers’ discretion in the absence of patient-related symptoms.
Outcome analysis
For the primary composite outcome, time to treatment failure, between-group comparisons will use the Mantel log-rank test, with magnitudes of treatment quantified by HRs (95% CI) obtained from Cox proportional hazard regression analysis. Alternatively, win probability by treatment will also be estimated to account for outcome hierarchy of surgery, hospitalisation, structural complication, severe symptoms and AEs, using methods similar to those in cardiovascular research literature, which have applicability for randomised trials in other therapeutic areas.46 Win probability quantifies the effect size as the probability that a participant in the switching arm will have a better change score (or win) over a participant in the continuation arm. For secondary outcomes, time-to-event outcomes will be analysed with Cox proportional hazard regression, binary outcomes will be analysed with the modified Poisson regression,47 and continuous outcomes will be analysed with linear mixed effects model for repeated measures.48 These analyses will be repeated in the per-protocol analysis set. All analyses will be adjusted for stratification factors used in the randomisation. Non-parametric methods will also be used to estimate win probabilities by treatment for binary, ordinal and continuous data.49
Safety analysis
Safety data for this study includes serious infections, defined as infections requiring hospitalisation and/or intravenous antibiotics. The primary safety outcome variable is the number of serious infections (eg, infections requiring hospitalisation and/or intravenous antibiotics) over 104 weeks of follow-up, analysed using the negative binomial regression. Hospitalisation due to complications of testing/monitoring and incidental cancer on advanced therapies will also be captured. Comparison of treatment effects will be conducted using the extended modified Poisson regression.50 Data on serious AEs (SAEs) will be presented by treatment group. Descriptive statistics will be presented, and no formal statistical tests will be performed because of data sparsity. SAEs will be summarised by the number and percentage of participants experiencing any SAEs, and any AEs leading to study drug discontinuation. Safety data will be presented by the treatment group.
Ethics and dissemination
The ethical considerations for such a study are important.51 The risks of treatments as identified in pivotal trials and in real-world experience are weighed against the risks of disease that is inadequately controlled, either because of subclinical inflammation that results in progressive complications of relapse or tissue damage, or if a switched therapy results in less efficacy than the index treatment or if it results in a drug-related or disease-related AE. Given that the risks of ‘silent’ inflammation and the benefits of mucosal healing which are associated with improved short- and longer-term outcomes, QUOTIENT was designed with this in mind, and with confidence that there is indeed clinical equipoise in this approach. The separate issue of patient autonomy and the discussions with patients about why a treatment change when they are feeling well may be warranted. As the field of IBD has moved to disease monitoring strategies that are available and visible to patients, the acceptability of treatment changes based on objective measures of disease activity is evolving. This study will add significantly to that conversation and inform patient educational materials as well. Results will be disseminated at scientific congresses and in peer-reviewed journals.
As of 19 December 2024, the current Institutional Review Board (IRB) approvals are Pro00077486; Pro00061437; STUDY00002062; 22-004171; i22-01269; IRB22-0890; IRB_00154397; 2000032384; SHIRB#2022.095-2; STUDY00007146; MMC#2024-18; REB#125290; 17784; Pro00142214; and 20240660-01H. Additional IRB approval information is available in online supplemental table 5.
Discussion
There is increasing emphasis on using the treat-to-target strategy to improve bowel healing and patient outcomes. Most providers and patients are comfortable with optimisation of an existing advanced therapy in efforts to treat-to-target; however, whether treatment should be switched to an alternative advanced therapy in pursuit of a treatment target of endoscopic/radiological remission presents clinical equipoise. The QUOTIENT study is designed to address this knowledge gap comparing two treatment strategies of treat-to-target in patients with IBD in symptomatic remission who have significant ongoing bowel inflammation, detectable by endoscopy/radiology.
No prior studies have addressed this specific clinical dilemma. In a cluster randomised trial, the Randomised Evaluation of an Algorithm for Crohn’s Treatment Study-2 (REACT-2), Jairath and colleagues compared the effectiveness of an enhanced-care algorithm incorporating early combination therapy and treatment intensification targeting absence of ulcers, to a step-care approach targeting clinical remission.52 In REACT-2, the investigators observed no difference in the risk of CD-related complications between treating to target of symptomatic remission versus treating to target of endoscopic remission. However, in a subset of patients with known active disease (known ulcers or elevated C reactive protein), treat-to-target of endoscopic remission decreased the risk of complications by 25%–30%, compared with a step-care approach. In contrast to prior trials like CALM and REACT-2, the patient population in QUOTIENT is asymptomatic with evidence of active inflammation on an advanced therapy. Moreover, the treatment strategy in QUOTIENT involves a potential ‘high-risk’ intervention, with switching to an alternative advanced therapy in patients who are feeling well (asymptomatic) on their existing advanced therapy.
Since QUOTIENT is a pragmatic trial being conducted in usual clinical practice, there are inherent differences from an explanatory trial. First, the primary and secondary outcomes are focused on patient-centred outcomes such as symptomatic remission, quality of life, treatment burden, and satisfaction. Achievement of endoscopic/radiological remission is not an outcome of the study, though this will be captured if endoscopy/radiology is being performed in routine care. Second, as a treatment strategy study, there is no mandate for a strict treatment algorithm regarding which patients receiving advanced therapies (who are randomised to switching) should be switched.53 In real-world settings, these decisions are variable, highly individual, and driven by the providers’ interpretation of evidence and experience on comparative effectiveness of different advanced therapies, patients’ preference for specific advanced therapies, and insurance coverage of different alternative advanced therapies. A limitation of this study is being underpowered for subgroup analyses, and several of those findings may be hypothesis-generating. In addition, medication adherence is measured using the participants’ medical records, which may not be as reliable as using a self-report adherence scale for self-administered therapies.
In summary, this pragmatic trial compares two treatment strategies of treat-to-target in patients with IBD who are asymptomatic but have evidence of ongoing significant bowel inflammation despite being optimised on their current therapy.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by list of Institutional Review Board approvals as of 19 December 2024: Advarra IRB (Central IRB), Baylor College of Medicine; Brown Gastroenterology Associates; Cornell; Dartmouth Hitchcock; Medstar Georgetown; Saratoga Schenectady Gastroenterology; University of Colorado; University of California San Diego; University of Texas Southwestern; Hoag Hospital; SSM Health Oklahoma; Gastro One; Massachusetts General Hospital; IBD Center of BC; and University of Texas Austin, IRB Reference numbers: Canada: Pro00077486; USA: Pro00061437. Cedars Sinai Office of Research Compliance and Quality Improvement, Cedars-Sinai, IRB Protocol ID: STUDY00002062. Mayo Clinic Institutional Review Boards, Mayo Clinic Jacksonville, IRB Application #: 22-004171. NYU Langone Health, Office of Science and Research Institutional Review Board, NYU Langone, Study Number: i22-01269. University of Chicago Biological Sciences Division IRB, University of Chicago, Protocol Number: IRB22-0890. The University of Utah Institutional Review Board, University of Utah, IRB Number: IRB_00154397. Yale Human Research Protection Program Institutional Review Boards, Yale University, IRB Protocol ID: 2000032384. Sutter Health Institutional Review Board, Palo Alto Medical Center, SHIRB #: 2022.095-2. University of Rochester Office for Human Subject Protection, University of Rochester Medical Centre, Study ID: STUDY00007146. Mercy Medical Center, Mercy Medical Center, Study ID: MMC#2024-18. Western Research, Western University, REB#125290. HiREB (Hamilton Integrated Research Ethics Board), McMaster University, REB#17784. UAlberta Health Research Ethics Board – Biomedical Panel, University of Alberta, Pro00142214. Pending exact name, local REB, McGill University, IRB # pending. OHSN-REB (Ottawa Health Science Network Research Ethics Board), Ottawa Hospital Research Institute, IRB# 20240660-01H. IRB, Institutional Review Board; NYU, New York University; REB, Research Ethics Board. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Medical writing support was provided by Kathleen Pillsbury, MPH, and Linda J Cornfield, PhD, ISMPP CMPP, of Alimentiv Inc. and was funded by Alimentiv Inc.
References
Footnotes
X @davidhudesmanMD, @Dana_Lukin, @ibdtweets, @vipuljairath
Contributors SS is the article guarantor. SS, VJ and JKH are responsible for conception and design. GZ provided formal data analysis. SS, JDN and JKH are responsible for project management/administration. SSi and JKH are responsible for supervision and manuscript drafting. SS, JDN, DIF, MEG, SAS, DH, RAM, DJL, ADF, CH, BS, JKJG, MCM, DTR, JGH, MM, TA, CM, FH, NN, TB, GR, JDM, ANA, RKC, JRRG, E-SG, SP, CAS, GYM, SAW, SP, GZ, VJ and JKH are all investigators, and have all made substantial contributions, reviewed/edited the manuscript for important intellectual content, and approved the final manuscript.
Funding This work was supported by Patient-Centered Outcomes Research Institute (PCORI), under contract CER-2020C3-21024. All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of PCORI, its Board of Governors or Methodology Committee. The study sponsor is the University of California, San Diego, with Baylor College of Medicine and Crohn’s & Colitis Foundation as collaborators.
Competing interests SS reports receiving research grants from Pfizer. DIF reports consulting/advisory board fees from Pfizer, Fresenius Kabi and Janssen. SAS reports being a consultant for Roche Information Systems. DH reports receiving research support from Johnson and Johnson and Pfizer; and consulting for AbbVie, Avalo, BMS, Corevitas, Eli Lilly, Johnson and Johnson, Pfizer, Prometheus, and Takeda. RAM has received consulting/advisory board fees from Pfizer, and received speaker’s fees from AbbVie, Takeda, Pfizer, Bristol Myers Squibb and Eli Lilly. DJL reports consultancy fees from Abbvie, Altrubio, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Johnson & Johnson, Palatin Technologies, Pfizer, Prime Therapeutics, Prometheus Laboratories, PSI, Takeda and Vedanta; has received speaker fees from AbbVie and Johnson & Johnson; and has received grants from AbbVie, Boehringer Ingelheim, Crohn’s & Colitis Foundation, Johnson & Johnson and Takeda. ADF has received consulting/advisory board fees from AbbVie; and reports receiving research support from Takeda. CH reports consulting/speaking with AbbVie, Janssen and Bristol Myers Squibb. JKJG reports receiving research support from Merck, AbbVie, Janssen, and Takeda. MCM reports speaking and consulting for Johnson and Johnson, AbbVie, Celltrion and Pfizer. DTR has received grant support from Takeda; and has served as a consultant for Abbvie, Altrubio, Apex, Avalo Therapeutics, Bristol-Myers Squibb, Buhlmann Diagnostics Corp, Celgene, Connect BioPharma, Intouch Group, Iterative Health, Janssen Pharmaceuticals, Lilly, Pfizer, Samsung Neurologica, and Takeda. He serves on the Board of Trustees for the Crohn’s & Colitis Foundation and is on the Board of Directors for Cornerstones Health. JGH has served on an advisory board for Bristol Myers Squibb. TA has received consulting or speaker fees from AbbVie, Takeda, Janssen, Ferring and Fresenius Kabi. CM has received consulting fees from AbbVie, Alimentiv Inc., Amgen, AVIR Pharma Inc., Bristol Myers Squibb, Celltrion, Eli Lilly, Ferring, Fresenius Kabi, Janssen, McKesson, Mylan, Pendopharm, Pfizer, Prometheus Biosciences, Roche, Sanofi, Takeda, Tillotts Pharma; speaker's fees from AbbVie, Amgen, AVIR Pharma, Alimentiv Inc., Bristol Myers Squibb, Eli Lilly, Ferring, Fresenius Kabi, Janssen, Organon, Pendopharm, Pfizer, Sanofi, Takeda, Tillotts Pharma; royalties from Springer Publishing; and research support from AbbVie, Ferring, and Pfizer. FH has served on advisory boards or as speaker for Abbvie, Janssen, MSD, Takeda, Pfizer, Celltrion, Teva, Sandoz, Amgen and Pendopharm; and has received independent research funding from Janssen, Abbvie, Pfizer and Takeda. NN has received honoraria from Janssen, AbbVie, Takeda, Pfizer, Merck, Sandoz, Novartis and Ferring. TB has received speaker or consultant fees from AbbVie, Alimentiv Inc., BMS, CSF Vifor, Eli Lilly, Ferring, Fresenius Kabi, Gilead, Iterative scope, Janssen, Merck, Mirium, Pendopharm, Pentax, Pfizer, Roche, Sandoz, Sanofi, Takeda, Viatris. GR has received honoraria as a consultant and/or speaker for Abbvie, Celltrion, Fresenius Kabi, Ferring, Janssen, Merck, Organon, Pendopharm, Pfizer, Takeda, Sandoz and Viatris; he has received Research Grant Support from Abbvie, Ferring, Pfizer, and Crohn’s and Colitis Canada; and he has received educational grant support from Celltrion, Pfizer and Takeda. JDM reports potential conflicts with AbbVie, Amgen, Celltrion, Fresenius Kabbi, Pfizer, J and J, Takeda and Eli Lilly. RKC reports consulting and participation in advisory boards for AbbVie, Adiso, BMS, Janssen, Pfizer, Magellan Health, Option Care, Pharmacosmos, Pfizer, Samsung Bioepis, Sandoz and Sebela; speakers bureau for Pfizer; research grant from Janssen; and is a member of the Executive Committee for the IBD Education Group and Scientific Co-Director of the CorEvitas Registry. CAS reports Consultant/Advisory Board for Abbvie, BMS, Boomerang, Buhlmann, Janssen, Lilly, Napo Pharmaceuticals, Pfizer, Prometheus Biosciences, Prometheus Labs, Takeda and Trellus Health; speaker for CME activities for AbbVie, Janssen, Pfizer and Takeda; grant support from AbbVie, Janssen, Pfizer and Takeda; and licensing fees for Takeda. GYM has received consulting/advisory board fees from AbbVie, Arena Pharmaceuticals, Boehringer-Ingelheim, Bristol Myers Squibb, Celgene, Dieta Health, Eli Lilly, Enthera, Ferring, Fresenius Kabi, Genentech, Gilead, Iterative Health, Janssen, Medtronic, Oshi Health, OptionCare, Pfizer, Prometheus Labs, Rippling, Shield Therapeutics, Shionogi, Takeda, Techlab, Verantos, Viatris; and research support from Pfizer. SAW is an employee of the Crohn’s & Colitis Foundation. GZ has received consulting fees from Alimentiv Inc. VJ has received has received consulting/advisory board fees from AbbVie, Alimentiv Inc., Altruboi, Amgen, AnaptysBio, Arena Pharmaceuticals, Asahi Kasei Pharma, Asieris, Astra Zeneca, Avoro Capital, Bristol Myers Squibb, Calluna Pharma, Celltrion, Eli Lilly, Endpoint Health, Enthera, Exeliom Biosciences, Ferring, Flagship Pioneering, Fresenius Kabi, Galapagos, Gilde Healthcare, GlaxoSmithKline, Genentech, Gilead, Innomar, JAMP, Janssen, Merck, Metacrine, Mylan, MRM Health, Mylan, Nxera Therapeutics, Organon, Pandion, Pendopharm, Pfizer, Protagonist, Reistone Biopharma, Roche, Roivant, Sandoz, Second Genome, Sorriso, Spyre Therapeutics, Synedgen, Takeda, TD Cowen, Tillotts, Topivert, Union Therapeutics, Ventyx, and Vividion; and received speaker’s fees from Abbvie, Ferring, Bristol Myers Squibb, Galapagos, Janssen, Pfizer, Takeda and Fresenius Kabi.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.