Article Text

Abstract
Objectives This study aimed to evaluate the real-world effectiveness of tofacitinib for treating moderate-to-severe ulcerative colitis (UC).
Design Systematic review and meta-analysis.
Data sources PubMed, EMBASE and Cochrane CENTRAL databases were searched from inception up to 18 July 2023. Reference lists of included studies were manually searched to identify potentially relevant studies not found in the databases.
Eligibility criteria Eligible studies included real-world observational studies, reported in English, on patients with moderate-to-severe UC treated with tofacitinib, defined by the Partial Mayo Score. Excluded were clinical trials, reviews, letters, conference abstracts, case reports and studies involving patients with mixed Crohn’s disease.
Data extraction and synthesis Two independent reviewers extracted data and recorded it in Excel. Quality assessment was performed using the Newcastle-Ottawa scale. Meta-analysis was performed using random-effects models due to high heterogeneity across studies.
Results 19 studies containing a total of 2612 patients were included. Meta-analysis revealed that clinical response rates were 58% at week 8, 61% at weeks 12–16, 51% at weeks 24–26 and 51% at week 52. Clinical remission rates were 39% at week 8, 43% at weeks 12–16, 40% at weeks 24–26 and 43% at week 52. Corticosteroid-free clinical remission rates were 33% at week 8, 37% at weeks 12–16, 32% at weeks 24–26 and 40% at week 52.
Conclusion This meta-analysis of real-world studies indicates that treatment of UC with tofacitinib is associated with favourable clinical response and remission rates in the induction and maintenance phases.
- CLINICAL TRIALS
- COLORECTAL DISEASES
- DRUG METABOLISM
- ULCERATIVE COLITIS
- META-ANALYSIS
Data availability statement
The data used in this systematic review and meta-analysis are derived from publicly available sources, such as published articles and reports. All data supporting the findings of this review are included within the manuscript.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Clinical trials have established the efficacy of tofacitinib in treating ulcerative colitis (UC). However, the relevance of these findings to real-world scenarios remains uncertain.
WHAT THIS STUDY ADDS
The systematic review and meta-analysis offers insights into the efficacy of tofacitinib in treating UC based on the latest real-world data. Notably, it extends the analysis of tofacitinib’s effects to 52 weeks post-treatment initiation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These findings provide clinicians and policy-makers with real-world evidence to guide treatment decisions and shape guidelines for UC.
Introduction
Ulcerative colitis (UC) is a recurring, chronic inflammatory bowel disease (IBD) characterised by mucosal inflammation that begins in the distal regions of the colon and can extend upward, ultimately affecting the entire colon.1 In 2023, it was estimated that UC affected approximately 5 million individuals globally, with a rising global incidence.2 While UC can manifest at any age, it most commonly occurs between the ages of 20 and 40, with roughly equal frequency in men and women.3 Traditional treatments for UC include mesalamine, glucocorticoids, immunomodulators and biologics offer relief to some patients.4 However, despite progress in treatment methods, clinical remission is only achieved in a relatively small number of patients.5
Tofacitinib has been approved by the US Food and Drug Administration for the treatment of UC. Controlled clinical trials have shown that oral tofacitinib is effective for treating UC in adults and is associated with high clinical response and clinical remission rates.6–10 Tofacitinib is a reversible, competitive inhibitor of Janus kinase (JAK), specifically targeting JAK1 and JAK3. Inhibition prevents the phosphorylation of JAK proteins, thereby blocking the activation of the STAT pathway and downstream signalling of cytokines such as interleukin (IL)-2, IL-4, IL-7, IL-15 and IL-21, as well as the production of proinflammatory proteins associated with mucosal inflammation.11
Although clinical trials have shown that tofacitinib is effective for treating UC and has an acceptable safety profile, findings from controlled trials are not always the same as when the drug is used in an uncontrolled clinical practice. Real-world studies can assess tofacitinib’s performance in diverse patient populations, taking into consideration factors such as demographics, comorbidities, concurrent medications and treatment adherence.12 Previous meta-analyses and systematic reviews, which have included data from real-world studies, have suggested that tofacitinib is a safe and effective treatment for UC. However, it is worth noting that the most recent studies included in these reviews only extended up to 2021. Additionally, few studies have examined the effectiveness of tofacitinib at 1 year after beginning treatment.13 14
Thus, our purpose was to perform a systematic review and meta-analysis of the effectiveness of tofacitinib for treating UC using only data from real-world studies. In addition, the analysis includes studies that provide outcome data at 1 year or more after beginning treatment.15
Methods
Search strategy
The current systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines15 (online supplemental file, PRISMA checklist). We conducted a comprehensive literature search of public databases including PubMed and EMBASE, for studies published from inception up to 18 July 2023. The specific keywords “tofacitinib”, “ulcerative colitis” and “real-world” were combined with Boolean operators and Medical Subject-Headings (MeSH) terms where appropriate were used in the searches to identify eligible studies. The exact search string used for PubMed and EMBASE was
Supplemental material
(tofacitinib OR XELJANZ) AND (“ulcerative colitis”) AND (real-world OR observational).
In addition, we conducted a handsearch of the reference lists in the included studies to identify any potentially relevant studies not identified in the database searches. Two reviewers independently screened the citations for eligibility to ensure accuracy and reliability in the selection process.
Selection criteria
This review was conducted following the PICOS criteria, which is based on participants (P), interventions (I), comparisons (C), outcomes (O) and study design (S). Eligible studies were those including patients with moderate-to-severe, active UC (P) who were treated with tofacitinib (I). The severity of UC is characterised by the Partial Mayo Score (PMS), which includes stool frequency, rectal bleeding and physician’s global assessment. Moderate-to-severe UC is typically defined by a PMS of 5–9. The comparator group could comprise patients on other JAK inhibitors, tumour necrosis factor inhibitors (TNFi) or none (C). The outcome of interest (O) was clinical remission rates, clinical response rates and corticosteroid (CS)-free clinical remission at the assessed time points. Only real-world observational studies with one or two arms were eligible for inclusion (S).
We excluded clinical trials, review articles, letters, commentaries, editorials, proceeding research, meeting abstracts, case reports and personal communications. Non-English studies, those involving tofacitinib combined with other biologics as treatment, and studies of patients with mixed Crohn’s disease were also excluded. Eligibility was confirmed by two independent reviewers, and any conflicts or uncertainties were resolved through discussion to reach a consensus.
Main outcome measures and data extraction
Primary outcomes were clinical remission rate and clinical response rate at various time points. Secondary outcomes were the CS-free clinical remission rate at given time points and adverse effects. Clinical remission was defined as a PMS of less than 3, with a combined stool frequency and rectal bleeding subscale score of 1 or less. Clinical response was defined as a reduction in the PMS by 3 points or more and at least 30% from baseline, along with a decrease of at least 1 point in the rectal bleeding subscale. CS-free clinical remission refers to a state in which a patient achieves and maintains clinical remission without the need for CS therapy.
Two independent reviewers read the full text of eligible articles, manually extracted the data and recorded it in Excel. Any inconsistencies were resolved through discussion. The following information was extracted from eligible studies, name of the first author, publication year, study design, country of the study, the number of patients with moderate-to-severe, active UC, mean patient age, the percentage of males, the mean follow-up duration and data regarding the outcomes of interest.
Quality assessment
The quality of the included studies was assessed using the Newcastle-Ottawa scale (NOS), following the recommendations of the Cochrane Non-Randomised Studies Methods Working Group.16 The NOS assigns a maximum of 9 points to each study, 4 points for the appropriate selection of patients, 2 points for comparability of participants in terms of design and analysis and 3 points for adequate outcome ascertainment. Two independent reviewers conducted the quality assessment, and any uncertainties were resolved through discussion.
Statistical analysis
The inverse-variance method, which is based on a weighted average of effect sizes from individual studies, was used to create forest plots displaying proportions with 95% CIs for individual studies and overall studies. Both fixed-effects and random-effects models were applied to calculate the pooled estimates presented in the forest plots. Heterogeneity among the studies was assessed using the I2 statistic, with the following criteria, 0%–24% indicated no heterogeneity, 25%–49% indicated moderate heterogeneity, 50%–74% indicated large heterogeneity and 75%–100% indicated extreme heterogeneity. Funnel plots were generated, and Egger’s test was applied to detect potential publication bias in the meta-analysis. The meta-analysis was performed using R-studio, and we used the R packages ‘meta,’ ‘dmetar,’ ‘metafor,’ ‘esc’ and ‘tidyverse.’ All analyses were two sided, and a value of p<0.05 was considered to indicate statistical significance.
Results
Search results
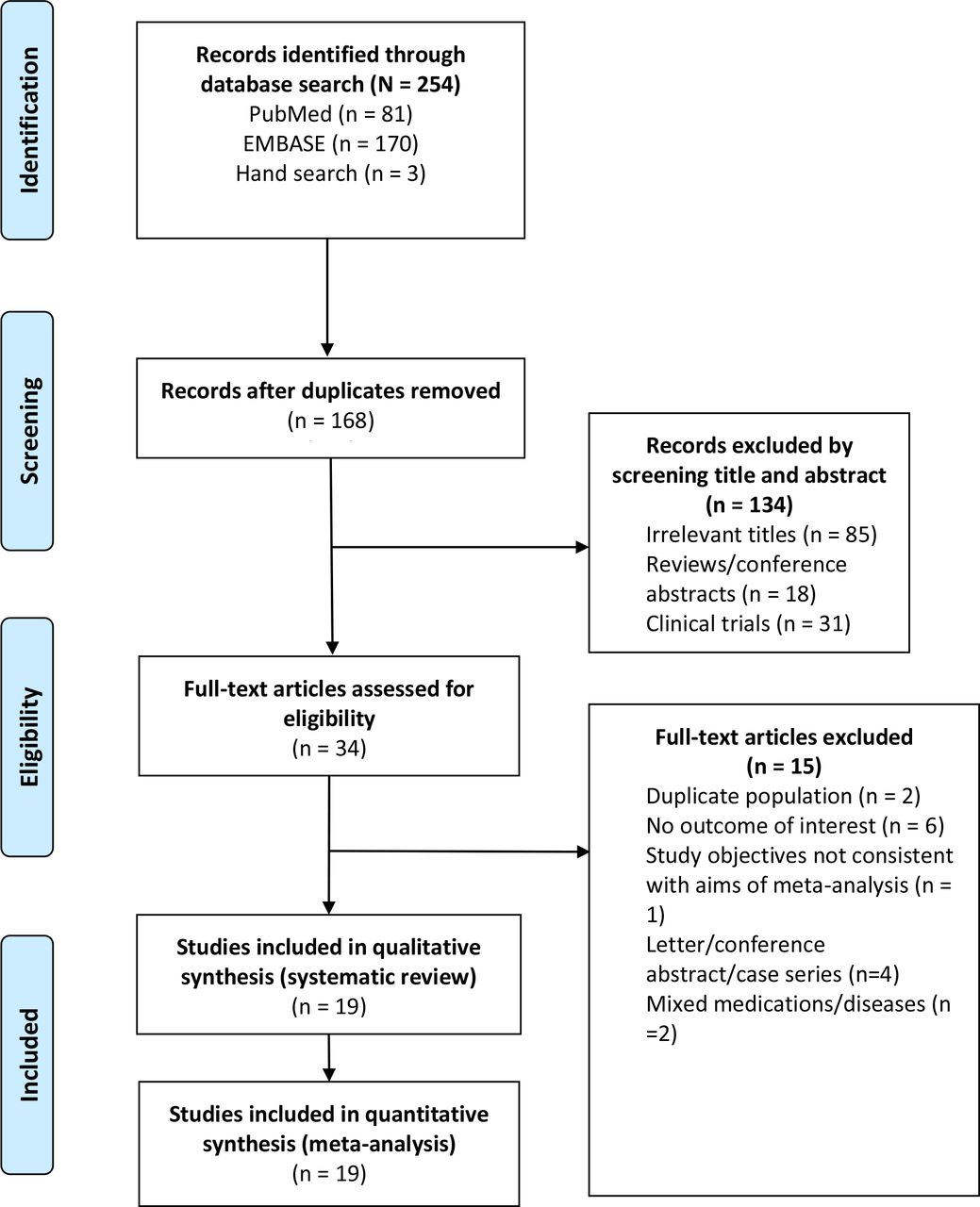
A flow diagram of the database search results and study inclusion is shown in figure 1. After the removal of duplicate entries, 168 potentially eligible studies were identified, and a preliminary screening of them was done based on their titles and abstracts. Subsequently, 34 full-text articles were assessed for eligibility, and 15 studies were excluded. Finally, 19 studies17–35 were included in the systematic review and meta-analysis.

A flow diagram of the database search results.
Characteristics of included studies
The 19 studies contained a total of 2612 patients with moderate-to-severe, active UC. The mean age of the patients ranged from 26.0 to 46.4 years, and the proportion of males ranged from 38.5% to 68.9%. All of the studies provided information regarding the proportions of patients with extensive disease or pancolitis, 15 studies reported data on patients previously exposed to anti-TNF treatments, 16 studies had information on patients with prior vedolizumab (VDZ) exposure, 13 studies included patients with prior ustekinumab (UST) exposure and 9 studies reported the proportion of patients who had received 2 or more prior biological treatments. The details of the included studies are summarised in table 1. The dose of tofacitinib is documented in online supplemental table S1.
Supplemental material
Characteristics of the included studies and patients
Meta-analysis
Clinical response
A total of 11 studies19–22 24 26 27 30 32 33 35 assessed the clinical response rate at various time points. Due to the heterogeneity (I2 ranging from 64% to 91%) across the studies, estimates by random-effects models were used as the pooled effect. The pooled estimates for clinical response rate were, 0.58 (95% CI 0.49 to 0.67) at week 8, 0.61 (95% CI 0.58 to 0.67) at weeks 12–16, 0.51 (95% CI 0.40 to 0.68) at weeks 24–26 and 0.51 (95% CI 0.26 to 0.77) at week 52 (figure 2).

Forest plots for clinical response rate at weeks 8, 12–16, 24–26, and 52.
Clinical remission
A total of 13 studies19–24 26 27 29 31–33 35 assessed the clinical remission rate at various time points. Due to the heterogeneity (I2 ranging from 71% to 78%) across the studies, estimates by random-effects models were used for the pooled effect. The pooled estimates for clinical remission rates were 0.39 (95% CI 0.31 to 0.44) at week 8, 0.43 (95% CI 0.37 to 0.49) at weeks 12–16, 0.40 (95% CI 0.32 to 0.48) at weeks 24–26 and 0.43 (95% CI 0.35 to 0.50) at week 52 (figure 3).

Forest plots for clinical remission rate at weeks 8, 12–16, 24–26 and 52.
CS-free clinical remission
A total of 12 studies18 20–22 24 25 27–30 33 34 provided data on the CS-free clinical remission rate. Due to the heterogeneity (I2 ranging from 74% to 88%) across the studies, estimates by random-effects models were used for the pooled effect. The pooled estimates for CS-free clinical remission rates were 0.33 (95% CI 0.24 to 0.41) at week 8, 0.37 (95% CI 0.29 to 0.45) at weeks 12–16, 0.32 (95% CI 0.23 to 0.41) at weeks 24–26 and 0.40 (95% CI 0.31 to 0.50) at week 52 (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots for CS-free clinical remission rate at weeks 8, 12–16, 24–26 and 52.
Safety
Due to the limited availability of data from only a few studies on serious adverse events (AEs) and infections, a quantitative synthesis could not be conducted. Specifically, Ma et al23 reported an AE rate of 9.6 serious AEs per 100 person-years, and Deepak et al17 reported a rate of 10.0 serious AEs per 100 person-years. Straatmijer et al18 reported a rate of 9.2 serious AEs per 100 person-years, and Shin et al29 reported a rate of 9.68 per 100 person-years. With respect to infections, Chaparro et al35 reported an infection rate of 1.67 per 100 person-years, and Ma et al23 reported a slightly higher rate of 2.1 infections per 100 person-years. Treatment discontinuation rates ranged from 12% to 56.1% among the 15 studies that reported this outcome (online supplemental table S2).
Publication bias
Funnel plots were created to assess the potential presence of publication bias. Three funnel plots were generated for the outcomes investigated, incorporating data from all study periods. Egger’s regression results suggested no evidence of publication bias, with p values of 0.12 for clinical response rate (online supplemental figure 1a), 0.17 for clinical remission rate (online supplemental figure 1b) and 0.46 for CS-free clinical remission rate (online supplemental figure 1c).
Supplemental material
Discussion
In this updated systematic review and meta-analysis focusing on the real-world use of tofacitinib for treating UC, tofacitinib demonstrated a strong clinical response rate of 61% and a remission rate of 43% during the initial phase of treatment. At 52 weeks, the clinical response rate was 51% and the remission rate was 43%. In addition, the pooled CS-free clinical remission rate in the induction phase was 37%, which increased to 40% at the 1-year follow-up. These results suggest that tofacitinib is an effective option for treating UC, with sustained improvements in UC symptom relief over time. However, the relatively high rates of treatment discontinuation in some studies underscore the need for individualised treatment approaches and ongoing research to optimise the use of tofacitinib for treating UC.
Tofacitinib is a small molecule inhibitor of Janus kinases (JAK), which include JAK-1, JAK-2, JAK-3 and TyK-2.36 37 Tofacitinib primarily inhibits JAK-1 and JAK-3 and is used to treat moderate-to-severe rheumatoid arthritis, psoriatic arthritis and IBD, including UC.36 37 The JAKs are important for immune activation and haematopoiesis, and the immunomodulatory effects of tofacitinib are a result of blocking these pathways.36 37 Risk stratification is important for the use of JAK inhibitors, including tofacitinib, as they may increase the risk of thromboembolic events, and major cardiovascular events in persons 50 years of age and older with pre-existing cardiovascular risk factors.37
Tofacitinib has become an important treatment for UC worldwide and is especially useful for patients in whom standard conventional or biological treatment have failed or who did not tolerate the treatment.38 A long list of studies has examined the effectiveness and safety tofacitinib for treating UC and other rheumatic conditions.38 This has resulted in multiple meta-analyses, mainly based on the results of clinical trials, examining its effectiveness and safety, and overall the studies have shown that tofacitinib is effective in treating UC with a good safety profile.
A few systematic reviews or meta-analyses using real-world data have been conducted previously, although with smaller sample sizes and shorter follow-up durations in comparison to the present study. Among, a prior real-world meta-analysis of the effectiveness of tofacitinib for treating UC was published by Taxonera et al.13 A total of 1162 patients with UC were included, and remission was achieved in 35% of patients at week 8 and 38% at month 6. The response rate was 62% at week 8 and remained high at 51% at 12 months. The incidence of serious AEs and herpes zoster per 100 patient-years was 8.9 and 6.9, respectively. However, that study did not assess 1-year clinical remission rate as evaluated in the present meta-analysis. Moreover, the mentioned meta-analysis incorporated conference abstracts, commonly considered ‘grey literature’, which could hinder the reliability of the pooled results.
Another real-world meta-analysis conducted by Lucaciu et al14 included 830 patients, of which 81% were previously treated with anti-TNF and 57% with VDZ.14 At week 8, 51% of patients achieved a clinical response and 37% remission. At 24 weeks, the rates were 40% and 29%, respectively. Still, the 1-year remission or response rate documented in the current meta-analysis was not reported by them.
Two other recent meta-analyses have found results similar to the two aforementioned studies. Taneja et al39 examined 26 studies in their meta-analysis and reported clinical response rates of 59% and 51% at week 8 and 1 years, respectively, and remission rates of 30% and 31%, respectively. The pooled incidence of AEs across all dosages was 4.4 per 100 patient-years, and a higher dose was associated with a higher frequency of AEs. CS-free remission rate was not assessed by them. That review also did not exclude meeting abstracts, and results from randomized controlled trials (RCTs) and real-world studies were combined together, possibly introducing bias into their findings. Lastly, Macaluso et al40 performed a meta-analysis of real-world studies that included 759 patients in seven studies. In contrast to our 1-year observation period, that review covered a temporal range of up to 24 to 26 weeks. At induction the clinical response rate was 49%, the clinical remission rate was 40%, and the CS-free clinical remission rate was 34%. Notably, the pooled incidence of AEs was high at 53.0 per 100 person-years, however, this may have been related to the criteria used in the analysis.
The OCTAVE Open trial examined the safety and effectiveness of tofacitinib for treating UC, with up to 7 years of treatment.41 In the analysis of outcomes by 12 months,9 the efficacy appeared to be better than the outcomes observed in the present meta-analysis of real-world studies. Specifically, after de-escalating tofacitinib, 84.1% sustained a clinical response at 12 months. In the dose escalation group, 64.9% had a clinical response by 12 months, with remission rates of 35.1% and 49.1% at the same intervals, respectively. The difference in observed efficacy between the OCTAVE Open and the present meta-analysis of real-world studies may stem from several factors. First, RCTs are conducted under controlled conditions with strict protocols, often resulting in higher efficacy. Second, RCTs generally involve more homogeneous patient populations, while real-world studies include a broader range of patients with varying stages of disease and comorbidities, which can impact outcomes. Third, patients in real-world settings may not adhere to treatment protocols as closely as those in RCTs, leading to lower observed efficacy.
In the final analysis of OCTAVE Open,41 81.5% of patients initially received tofacitinib 10 mg two times per day. By month 36, clinical response rates were 66.9% for patients on 5 mg and 40.3% for those on 10 mg, with endoscopic improvement seen in 64.6% and 37.1%, and remission maintained or achieved in 58.9% and 33.7%, respectively. With regard to AEs, the incidence rates (2440 patient-years) were death, 0.25, serious infections, 1.61, herpes zoster (all), 3.16 (2.47–3.97), opportunistic infections, 0.87 and major adverse cardiovascular events, 0.16. The incidences of other AEs studied were all ≤1. Discontinuation occurred in 48.0% of patients in the tofacitinib 5 mg bid group and in a much higher proportion, 86.5%, in the tofacitinib 10 mg bid group. Notably, 22.4% of patients in the 10 mg bid group discontinued by month 2 due to insufficient clinical response. The study conclusion was that tofacitinib demonstrated consistent safety up to 7 years.41 Another recent study examined up to 7.8 years of safety data from the Global Clinical Programme for the treatment of UC with tofacitinib.42 The incidence rates of AEs were similar to those reported in the aforementioned study, deaths, 0.23, serious infections, 1.69, herpes zoster (all), 3.30 and opportunistic infections, 1.03. Notably, the incidence of major cardiovascular events was 0.29, deep vein thrombosis was 0.03 and pulmonary embolism was 0.19.
According to our review, treatment discontinuation ranged from 12% to 56.1% across the studies that reported this outcome. The reasons for tofacitinib discontinuation poststudy enrolment varied. For example, several studies documented that non-response, or a lack of initial therapeutic effect, led to discontinuation as continued treatment was deemed ineffective.18 19 21–23 31 In other cases, AEs such as serious infections, rash and anaemia necessitated discontinuation due to safety and tolerability concerns.17–22 24–28 31 33–35 Additionally, loss of response, characterised by initial improvement followed by regression, prompted a strategic reassessment of treatment and subsequent discontinuation.18 21 26
Another important issue is that, across different outcomes, moderate to large heterogeneity was detected among the studies. This variability likely stems from differences in demographics and treatment histories among the included studies. Such variations challenge the robustness of our interpretations. Additionally, there was significant variability in the patients’ treatment histories, particularly concerning prior exposures to anti-TNF agents, VDZ and UST. These factors might also contribute to the observed heterogeneity. Accordingly, future meta-analyses should consider conducting subgroup analyses to address this heterogeneity when more studies become available.
Strengths and limitations
The primary strength of this meta-analysis is its comprehensive inclusion and analysis of real-world data, offering insights into the effectiveness of treatment at various time points up to 1 year after beginning treatment. In addition, the meta-analysis included approximately 2600 patients, a more than threefold increase compared with the previous analysis by Lucaciu et al14 and more than double the number of patients in the review by Taxonera et al.13 However, notable heterogeneity among the included studies across the outcomes evaluated is a significant limitation of the present meta-analysis. Further, the exclusion of grey literature represents a trade-off. While it can be considered a strength by focusing on peer-reviewed studies only, it may also lead to publication bias, as it potentially omits studies reporting negative or less significant results. Retrospective studies can introduce selection bias, which is a limitation of this meta-analysis.
Conclusion
This updated meta-analysis supports tofacitinib as an effective treatment for UC in the real world, particularly high clinical response and remission rates during the induction phase and the maintenance period, indicating its potential for long-term symptom relief. Additional meta-analyses to quantitatively synthesise the long-term safety outcomes are highly recommended.
Data availability statement
The data used in this systematic review and meta-analysis are derived from publicly available sources, such as published articles and reports. All data supporting the findings of this review are included within the manuscript.
Ethics statements
Patient consent for publication
Ethics approval
This systematic review and meta-analysis did not use raw patient data or private information. As a result, there was no requirement for approval of the protocol by the hospital Institutional Review Board (IRB) or for patient informed consent.
References
Footnotes
CW and H-HW contributed equally.
Contributors C-HL: conception and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript; statistical analysis; literature research; administrative, technical or material support; supervision. W-SL: acquisition of data; analysis and interpretation of data; critical revision of the manuscript; administrative, technical or material support; supervision; guarantor of integrity of the entire study. CW: conception and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript; administrative, technical or material support; supervision. H-HW: conception and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript; literature research; administrative, technical or material support.
Funding NSTC: 107-2314-B-075-036, 108-2314-B-075-043 -MY2, 110-2314-B-075-017, 111-2314-B-075-046-MY2; VGH: V111C-177, V112C-177, V113C-174.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.